A TELEMEDICINE PATIENT CENTRED DOCUMENTATION
A note before we begin :
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs .This e-log book also reflects my patient centered online learning portfolio and your valuable comments on comment box is welcome.
What the readers can expect from this piece of document :
This case was a telemedicine based one whereby , I ( under the guidance of my teacher ) tried to converse, understand the problem being faced by the patient and advice her regarding the relieving measures ( while mentioning her to consult a physician or a nearby health care institution in case of emergency )
this is a CONVERSATIONAL E-LOG
i.e I shall sequentially arrange the learning conversation that went on between the mentor and mentee..to project and highlight how one single patient can trigger thousands of learning possibilities and open up innumerable closed doors to lead to the pinnacle of knowledge.
DEIDENTIFICATION : Please note that the participants of the conversation have been deindentified
HP : Mentor
MN : Mentee
[10:09 AM, 7/1/2021] Mentor : Can any of our student members here take the details of a middle aged woman told to have a BP that is very low, pulse thready with borderline diabetes so that we can understand her current requirements and then advice her?
A similar exercise was recently carried out in this group and archived here https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.html?m=1
Pm me for her phone number if anyone is interested in the above exercise of improving learning outcomes to drive real patient health outcomes
[10:09 AM, 7/1/2021] Mentor: 👆if you are planning to call her later she would prefer evening
[10:09 AM, 7/1/2021] Mentor: Some literate pateints can even be texted
[10:09 AM, 7/1/2021] Mentee: Ok sir
Will call her in the evening.
[10:09 AM, 7/1/2021] Mentee: Sir
The patient you had spoken to yesterday...
The referral
She has bp of 110 /60
[10:09 AM, 7/1/2021] Mentor: Feedback from my friend (who is also her friend)
"Spoke to the Dr student. Thanx i felt better just speaking to her "
Well done 👏
[10:09 AM, 7/1/2021] Mentor: Very well done audio as well as overall consultation.
I think it will be a good idea to make some audio case reports (first time in the world?) and E log them to share them widely as learning insights into Telemedicine. Take a signed informed consent for it if possible although the patient is already perfectly deidentified here so it may not be necessary. You can even try audio visual consent taking as it would gel with the national bioethics research guidelines
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5799953/
[10:09 AM, 7/1/2021] Mentee: Her blood pressure today is 104/72 mm Hg
[10:09 AM, 7/1/2021] Mentee: Sir
I told her not to take antihypertensive meds today as well
Maybe we can start from tomorrow
[10:09 AM, 7/1/2021] Mentor: Ask her to monitor it regularly and take it only if it goes above 135/85 among the average of all her daily readings.
Maybe she never needed the antihypertensives in the first place? How long has she been told to have hypertension?
[10:09 AM, 7/1/2021] Mentee: For the past 3 years sir
[10:09 AM, 7/1/2021] Mentor: Let's monitor and see.
Maybe she never needed it
[10:09 AM, 7/1/2021] Mentee : Sir
Her b.p. is being somewhere around 120/70 mm Hg
[10:09 AM, 7/1/2021] Mentee: But it has been more than a week she is without her meds
[10:09 AM, 7/1/2021] Mentee: Should we start her on half dosage of what she used to have previously sir?
[10:09 AM, 7/1/2021] Mentor: Let's ask her to monitor and let us know how many times it's going above 140'/90.
She needs to monitor at least ten times a day at random intervals
[10:09 AM, 7/1/2021] Mentee: Ok sir
[10:09 AM, 7/1/2021] Mentee: She usually takes this antihypertensive combination sir( telmisartan + Chlorthalidone )
[10:09 AM, 7/1/2021] Mentor : The chlorthalidone can cause dangerous hyponatremia
[10:09 AM, 7/1/2021] Mentee: Yes sir!!
Even telmisartan proves to be too sensitive to many patients sir
Y not keep her on losartan twice daily?
[10:09 AM, 7/1/2021] Mentor: Anyway she is not that much of a hypertensive
[10:09 AM, 7/1/2021] Mentee And because of the long acting effect of Telma she is having these readings maybe
[10:09 AM, 7/1/2021] Mentee: And even after that if she needs titration we can add a beta blocker once daily
[10:09 AM, 7/1/2021] Mentee: That too she is on telmisartan 80 mg !!!
People get hypotensive phases with 40 mg itself sir!!
[10:09 AM, 7/1/2021] Mentee: That patient
[10:09 AM, 7/1/2021] Mentee: Developed pedal edema as well
[10:09 AM, 7/1/2021] Mentee: Pitting type till the ankle
[10:09 AM, 7/1/2021] Mentee : I guess the chlorthalidone was helping her edema till now.
Mentor :What may have been the cause for her edema? Hypoalbuminemia or heart failure or idiopathic edema of women?
[10:09 AM, 7/1/2021]Mentee: We need to get investigations done for that..
[10:09 AM, 7/1/2021]Mentor: Before that can we have her history from earlier let's say from the time she first met a doctor and was detected hypertensive or even earlier from her childhood?
[10:09 AM, 7/1/2021]Mentee : Ok sir
[10:09 AM, 7/1/2021] Mentee:Will talk to her today
[10:09 AM, 7/1/2021] Mentor: Chest X-ray
Ecg
Echocardiography
(even in the past if available)
Video of her neck veins in the 90 degree sitting position
Serum albumin (even in the past if available)
[10:09 AM, 7/1/2021] Mentee: Ok sir
Urea
Creatinin?
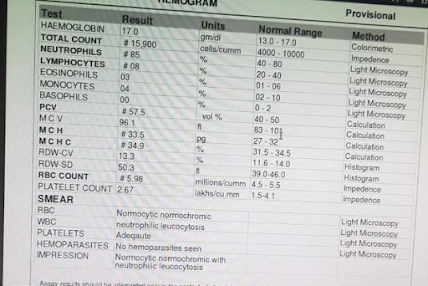
[10:09 AM, 7/1/2021]Mentor: Any past report of complete hemogram
[10:09 AM, 7/1/2021] Mentor: Yes just creatinine will do
[10:09 AM, 7/1/2021] Mentee: Okkay sir
[10:09 AM, 7/1/2021] Mentee: Sir
[10:09 AM, 7/1/2021] Mentee: That patient
[10:09 AM, 7/1/2021] Mentee: She got dyspneic
[10:09 AM, 7/1/2021] Mentee: Maybe coz of the fluid overload!
[10:09 AM, 7/1/2021] Mentee: She has a history of huge steroid intake
[10:09 AM, 7/1/2021] Mentee: To treat her psoriasis
From a naturopathy doctor
[10:09 AM, 7/1/2021] Mentor: Possible heart failure.
Why was she on steroids?
[10:09 AM, 7/1/2021] Mentor: How do we know it was steroids as naturopath doctors are not supposed to be prescribing it
[10:09 AM, 7/1/2021] Mentee: I told her to resume her medicine
And in the mean time get the investigations done
[10:09 AM, 7/1/2021] Mentee: No sir
It's a long story
I will tell you completely ,give me some time sir
I ll talk to her some more
[10:09 AM, 7/1/2021] Mentor: Hope you asked her to remain in touch with a local physician in case of emergency
[10:09 AM, 7/1/2021] Mentor: When did she first notice her psoriasis? When did the tea company doctor first prescribe her medications for her ankle swelling? Was the dyspnoea noticed by her today for the first time?
[10:09 AM, 7/1/2021] Mentee: Ans 1. 3 years back
Ans 2. Around 2 back.
Ans 3. Today.
[10:09 AM, 7/1/2021] Mentee: *2 years
[10:09 AM, 7/1/2021] Mentor: No past history of asthma?
What drugs did the previous doctor prescribe two years back? How long did she take them?
[10:09 AM, 7/1/2021] Mentee: Goodevening sir
Sir that lady...your colleague's acquaintance..
She has given her blood sample for investigation..
Reports awaited..
The technician has said after doing the ecg and 2D echo that all is fine it seems
Though official report and strip is awaited .
She had resumed taking her medication due to the fluid accumulation..edema..and SOB
But her b.p is low only sir ..
110/60 mm Hg on an average
Could u help me regarding what I should comment about her taking the meds and the existing low b.p
[10:09 AM, 7/1/2021] Mentor: 110/60 should be OK.
She should just take care it doesn't fall below 80/50
[10:09 AM, 7/1/2021] Mentee: Sir
One more thing I wanted to share with you
Remember the patient who was your friend's friend..
The lady with low B.p ?
She used to send him her b.p.readings every morning..and update about her health and all
Once the topic of the locations of residences had come up
And then yesterday she sent me a cake which she had herself baked.
[10:09 AM, 7/1/2021] Mentee: I felt so humbled
I told her many times that her regard was enough ,the cake wasn't needed at all
But she had already baked and sent it
[10:09 AM, 7/1/2021] Mentor: Tell her to send healthy fruits and vegetables next time as cakes and all other baked products are unhealthy and possibly responsible for her hypertension and other NCDs that emerge from the visceral fat driven adipokines.
[10:09 AM, 7/1/2021] Mentee:
She is home baker sir.. she finds joy in baking.. maybe I ll make her sad if I tell her to stop her hobby :( but definitely I tell her not to consume her bakery products :)
[10:09 AM, 7/1/2021] Mentee: Sir
Thankyou for letting me have the opportunity to interact with my patients
To understand them
And to get all the love from them
[10:09 AM, 7/1/2021] Mentor: This is psychotherapeutic redirecting challenge. Take up this challenge with Mahima to redirect her cooking joy in a healthier direction?
[10:09 AM, 7/1/2021] Mentee: Will try sir.