I am Saranya ,a final year MBBS student.
Greetings to all my readers;
This is an elog documenting the patients that I witness during my Clinical Postings to enforce a greater patient centered learning .
I shall be presenting and discussing this patient as a part of my Prefinal Examination General Medicine Assessment process.
DEIDENTIFICATION :
The privacy of the patient is being entirely conserved. No identifiers shall be revealed through out the piece of work whatsoever. CONSENT obtained.
I thank Dr. Simran Ma'am (intern) for helping me understand more about this case
This case is about a 29 year old lady residing in a village in the southern part of India ,who takes care of her household and she came to us to seek help for
Chief Complaints :
- B/L joint pains (knees) since 10 months
- B/L itching in the upper aspect of chest and neck since 10 months
DAILY ROUTINE OF THE PATIENT :
The patient lives in a family of 3 ..(of late the family has expanded) which constitutes her husband ,her mother in law and herself . They follow Islam.
A usual day in her life :
4.40 am : wakes up and bathes
5.00 am : Prayer
5.15 am : She doesn't sleep but lies on her bed and rests for another one or two hours since the work load is not enough in the household to begin her chores at 5 am itself
7.30 am : washes dishes from the last day, washes clothes, makes the morning tea for herself and her family members
9.00am : gets food ready for her husband who goes out for work after breakfast
9.30 am : Serves breakfast for her mother in law and herself
Rests for a while
11.00 am : Prepares for the day's cooking
Rests for a while
12.00 noon : cooks for the day
1.00 pm : Serves lunch for her husband who comes back during afternoon
2.00 pm : Serves lunch for her mother in law and herself
3.00 pm : Rests
4.00 pm : Prayer
5.00 pm : Makes tea for everyone in the house
In the evening mostly all of them sit down and watch television
7.00 pm : Preparations for dinner
8.30 pm : Serves dinner for the family and then for herself
10.00 pm : Sleeps
How the Disease affected and changed her daily life
The disease manifested almost around January last year when she began having joint pains,
At the level of her daily life ,she expresses she began feeling tired and fatigued very easily
Where by after very short spans of work or chores she felt like lying down and taking some rest before the next work ,
Whenever she did a little bit of work , her joints seemed to become " tight " and painful .
The Lassitude was to an extent so much so that she yearned that there was someone who would get everything ready for her and get it for her at bed itself such that she wouldn't have to get up.
Please note : The words have been put just as expressed by the patient such that the intensity and nature of her problem is interpreted better .
HISTORY OF PRESENTING ILLNESS : Around 10 months ago she developed symmetrical b/l joint pains in the knees which was insidious in onset, gradually progressive, no aggravating factors and relieved on medication i.e. TAB. HYDROXYCHLOROQUINE 200 mg (suggested by a local physician)
Around the same time she developed itching over neck and upper chest area. As a result of the itching, the area was initially red and turned black.
C/O Alopecia since 10 months. It was gradually progressive leading to severe hair loss over the past 10 months. Associated with thinning of hair.
C/O bilateral pitting type of pedal Edema and Edema over the dorsal aspect of hands.
C/O generalised pain.
C/O Difficulty in walking.
C/o weakness
C/O distal muscle weakness manifested in the form of : difficulty in mixing food, eating with hands, buttoning-unbuttoning of shirt, combing of hair.
C/O proximal muscle weakness manifested in the form of : difficulty in getting up from squatting position, getting objects present at a height.
C/O Dyspnea on exertion (NYHA- 3), gradually
progressive since 4-5 months.
C/O vaginal discharge since 7-8 months.
Past h/o: She has not experienced similar joint pains or itching in the past.
Menstrual h/o:
Attained menarche at 12 years of age , 3/25-28, regular , no pains, no clots.
Marital h/o:
Non consanginous marriage , married life of 14 years , Primary infertility (Nulligravida)
Has recently adopted a girl from her sister-in-law.
Family h/o: No similar complaints in the family
Personal h/o:
Diet- Mixed
Appetite- Decreased
Sleep- Inadequate since 10 months
Bowel and bladder habits- Regular
No addictions
No known drug allergies
General physical examination: The patient is conscious, coherent, cooperative well oriented to time, place and person. She is moderately built and moderately nourished.
Pallor- present

No icterus, cyanosis, clubbing, lymphadenopathy.
Pedal Edema- present

O/E:
- Diffuse mottled erythematous hyperpigmentation (Heliotrope rash) noted on B/L cheeks, nose(bridge) involving nasolabial folds, ears, neck extending onto upper chest and back forming a ‘V’ on anterior chest (Shawl sign).



- Few hyper-pigmented macules noted on mid and lower back (‘V’ sign).

- Single erythematous macule noted over the right loin (Holsier sign).

- Pigmentation of B/L knuckles noted (Gottron’s Papules).


Vitals:
Temperature- Afebrile
BP- 130/80 mm Hg
PR- 102 bpm
RR- 14 cpm
SpO2- 99% @ RA
SYSTEMIC EXAMINATION:
CVS- S1, S2 sounds heard. No murmurs
RS- BAE+ NVBS heard
CNS- NAD
P/A- Soft, non tender, Bowel sounds heard
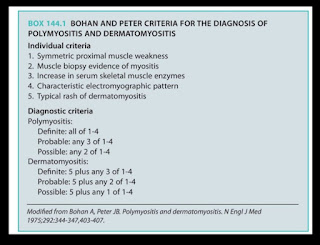
Provisional diagnosis:
DERMATOMYOSITIS WITH PRIMARY INFERTILITY
GENITAL CANDIDIASIS
?SLE
DVL REFERRAL WAS TAKEN-


INVESTIGATIONS:



Serology - Negative
RA Factor- Negative
CRP- Negative
TREATMENT :


STUDIES
: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5715209/
( about management options ( protocol of therapy and advantage of systemic drugs in cutaneous manifestations )
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5952016/
( Antimalarial drugs in Dermatomyositis )
https://advancesinrheumatology.biomedcentral.com/articles/10.1186/s42358-020-00134-8
( Efficacy of hydroxychloroquine )
https://academic.oup.com/rheumatology/article/41/1/7/1787912
(Treatment options)
https://www.sciencedirect.com/science/article/pii/S2589909019300188
( Bohan and Peter Criteria for Dermatomyositis )
No comments:
Post a Comment