I am
Saranya ,a final year MBBS student.
Greetings
to all my readers;
This is an
elog documenting the patients that I witness during my Clinical Postings to
enforce a greater patient centered learning .
DEIDENTIFICATION :
The privacy of the patient is being entirely
conserved. No identifiers shall be revealed through out the piece of work whatsoever.
Introduction :
Here we shall discuss our patient who is a 38 year
old lady hailing from a village in South India .She is a tailor by occupation.
Presenting
Picture of the patient :
BACKGROUND
Almost all her 38 years of life have been if a different shade as compared to any other of her contemporaries.
This is because when she was 3 year old ,one day she experienced fever for a day and then the next day she developed inability to move both her lower Limbs.
Since then she has grown up with the help of mechanical support to substitute
her lost power in her lower Limbs.
Fast Forwarding
to 20 days before the day of presentation to our Hospital ( henceforth shall be
referred to Hospital2)
She developed
high grade fever , cough with sputum , headache.
She took medications
prescribed by a local physician
After a couple
of days , since any of the symptoms mentioned above weren’t subsiding
She was taken
to a local hospital ( Hospital1 )
There the attenders
were told that she has low hemoglobin ( 5gm/dl ) and was transfused 3 units of packed
cells .
Post other medications
administered by Hospital 1 her fever subsided but other problems did not.
4 days prior
to presentation to Hospital 2
She developed
weakness in her Right upper limb and Right lower Limb , slurred speech and disorientation.
She also had
seizure episode that night and couple of days even after that.
She was taken
to the same Hospital1 once again where they
referred her to Hospital 2 and thus she presented to us.
Note : No seizure
episode has been witnessed since admission to Hospital2 on 30.10.21.
DESCRIPTION
OF THE DAY THE PRESENT ILLNESS DEVELOPED :
Since she was
not keeping well since the last 20 days ,her husband used to keep a check on her
health via telephone from his workplace ( a restaurant cook )
On his call
that day , she mentioned to him that she wasn’t feeling quite well ,and by the time
he returned home after work ,he reports that her eyes had a blank stare , she could
identify him but she spoke few words which were slurred ,did not carry any meaning
and then she stopped speaking .
Some time later
she threw a seizure episode wherein her husband gives history of eye rolling and
tongue bite.
After which
she was taken to Hospital 1 and then Hospital 2.
CHRONIC
DISEASES :
She is not
a known case of DM ,HTN ,Bronchial Asthma ,TB, Thyroid.
DAILY
ACTIVITIES :
She consumes mixed diet , with a slightly lessened appetite since the past fortnight , sleeps adequately , bowel and bladder Normal
No history of any involuntary passage of urine or stools
She is not a smoker ,she doesn’t consume alcohol.
No known food or drug allergies.
FAMILY HISTORY :
No similar complaints in any of her immediate family members.
No history of sudden deaths in the family.
EXAMINATION
General examination :
Positive findings :
Pallor present.
Generalized edema present.
Hyperpigmented knuckles.
VITALS :
Body temperature: Afebrile
Pulse : 80 bpm
B.P : 130/70 mm Hg
R.R. : 16 bpm
On auscultation :
S1 , S2 heard.
Diffuse wheeze heard in all lung fields.
Abdomen soft and non tender.








R L
TONE UL Hypotonic Normal
LL Hypotonic Hypotonic
POWER UL 1/5 3/5
LL 1/5 2/5
REFLEXES
B T
S K A P
R 1+ - - - - Extensor
L 1+ 2+ - - - Extensor
Babinsky Positive in Right limb.
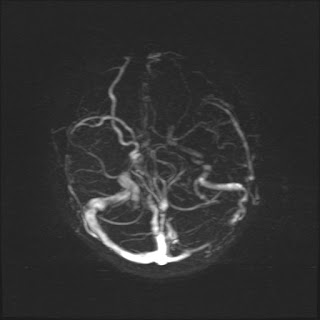
INVESTIGATIONS :









No comments:
Post a Comment