I am Saranya ,a final year
MBBS student.
Greetings to all my readers;
This is an elog documenting the
patients that I witness during my Clinical Postings to enforce a greater
patient centered learning
I will be presenting this case report
as my short case for my MBBS Final year Practical Examinations and viva voce scheduled to be held on 14th
June 2022
DEIDENTIFICATION :
The privacy of the
patient is being entirely conserved. No identifiers shall be
revealed through out the piece of work whatsoever.
CONSENT :
An informed consent has been taken from the patient in the presence of the family
attenders and other witnesses as well and the document has been conserved
securely for future references.
ACKNOWLEDGMENT
I
convey my regards to Dr. CHANDANA Ma'am ( Resident ,
Department of General Medicine ) for
guiding me regarding the case .
Documentation
:
is
being done on 12th of June 2022
(Updates
will be done later in the future with dates mentioned for the same.)
INTRODUCTION
:
My
patient is a 29 year old man , resident
of a rural district of South India
CHIEF
COMPLAINTS :
He presented with the complaints of
1.Fever since 5 days
2.Shortness of breath since 5 days
3. Decreased urinary output since 4 days.
History of Presenting illness :
TIMELINE :
1 year Back
The patient was asymptomatic 1 year back when he developed shortness of breath.
Visited Heath care centre
Was diagnosed with a lot of de novo findings
Failing kidneys
Diabetes Mellitus
Hypertension
Medications : Oral medications given for his kidney ailment was taken for 6 months and then stopped.
Antihypertensive and oral hypoglycemic were not taken.
1 month ago
Relapse of Shortness of Breath.
Hospitalized, hemodialysis done.
Discharged on 2nd of June 2022
7th June 2022
Patient developed high grade fever, with chills.
There is also history of cough,hemoptysis on Day 1 of the fever, did not happen again.
OTHER EXISTING PROBLEMS :
Bilateral Pedal Edema since 5 days
Decreased urine output since 3 days
Decreased appetite since 3 days
Decreased Sleep since 3 days owing to Shortness of Breath
Regular consumer of alcohol since 10 years, drinks about a quarter 4 times a week
No other addictions
DAILY ROUTINE : The patient is an auto driver by occupation but he was asked to reduce his work life due to his ailments ,nevertheless he continued to drive his vehicle, but has stopped completely since one month back,
Usually before his ailment he used to get up in the morning ,freshen up, have his breakfast and leave for work, lunch was usually done outdoors,evening times after returning from work he used to spend time with his friends ,after which he usually had dinner late at around 11 pm and then go to bed.
FAMILY HISTORY
No similar complaints in family
GENERAL PHYSICAL EXAMINATION
I have examined the patient after obtaining informed consent and providing reassurance ,in the presence of an attendant.
Examination has been done under adequate lighting ,with appropriate exposure , in both supine and sitting posture.
Privacy of the patient has been secured.
Findings:
· The patient is conscious, coherent,oriented to time,space and person , cooperative .
·mmoderately built and nourished
Findings : Mild Pallor
No cyanosis,clubbing,
Peno pedal edema
Jvp is not raised
C



VITALS
HR: 121 beats per minute
BP: 150/96 mmHg
RR: 24 cycles/minute
Temperature: 99 degrees. F
SYSTEMIC EXAMINATION :
CARDIOVASCULAR EXAMINATION :
Inspection :
Precordium :
No precordial bulges.
No engorged veins.
No scar/sinus.
No Visible pulsations :
Other findings :
Apex Beat : appears to be at the 6th Intercostal Space 1cm lateral to midclavicular line.
Chest wall Defects : None.
PALPATION :
Inspectory finding of Apical beat correlated on Palpation, can be localized 1cm lateral to the midclavicular line in the 6th Intercostal Space
PERCUSSION :
Cardiac Dullness
AUSCULTATION :
S1 ,S2 heard.
RESPIRATORY SYSTEM :
AUSCULTATION:
Bilateral air entry positive
Bilateral basal coarse crepts heard
Vocal resonance: resonant in all areas
Abdominal Examination :
P/A soft,non tender
No organomegaly.
CENTRAL NERVOUS SYSTEM :
Motor and Sensory functions intact,
No evidence of any focal neurological deficits.
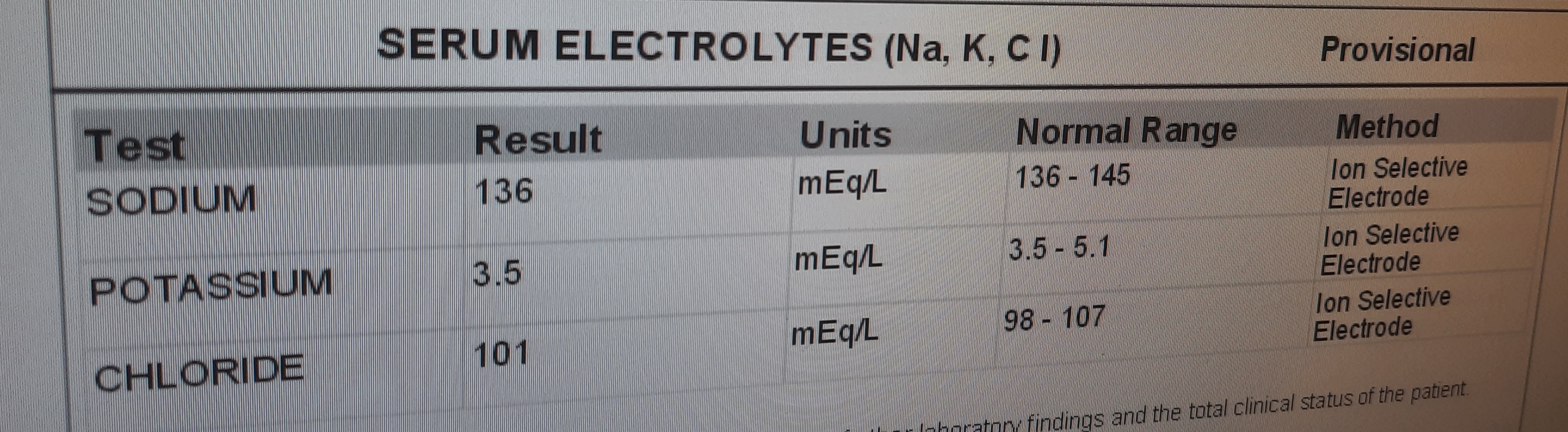
FEVER CHART AND INVESTIGATIONS :








PROVISIONAL DIAGNOSIS :
Diabetic and Hypertensive patient with alcoholism behaviour, PROBABLE CASE OF Heart failure secondary to ? INFECTIVE ENDOCARDITIS Along with existing CHRONIC KIDNEY DISEASE.
TREATMENT :
Hemodialysis
Inj. PIPTAZ 2.25gm IV TID
-Inj. LASIX 40mg IV TID
-Inj EPI 4000U SC weekly once
-T. Nodosis 500mg PO BD
-T. Orofex XT PO BD
-T Shelcal 500mg PO OD
-T. met XL 50mg PO BD
-Salt and fluid restriction
-Vitals monitoring 4hourly
-GRBS monitoring 12 hourly